The PulsePen tonometer was validated versus invasive method 1, 2 and versus MRI method.3
The PulsePen tonometer is one of the three devices used by the Stiffness Collaboration to establish the normal and reference values of PWV in healthy people.4
The reference values of PWV in children and teenagers were obtained using the PulsePen tonometer.5 In this study the PWV was evaluated in Algerian, Hungarian and Italian populations.
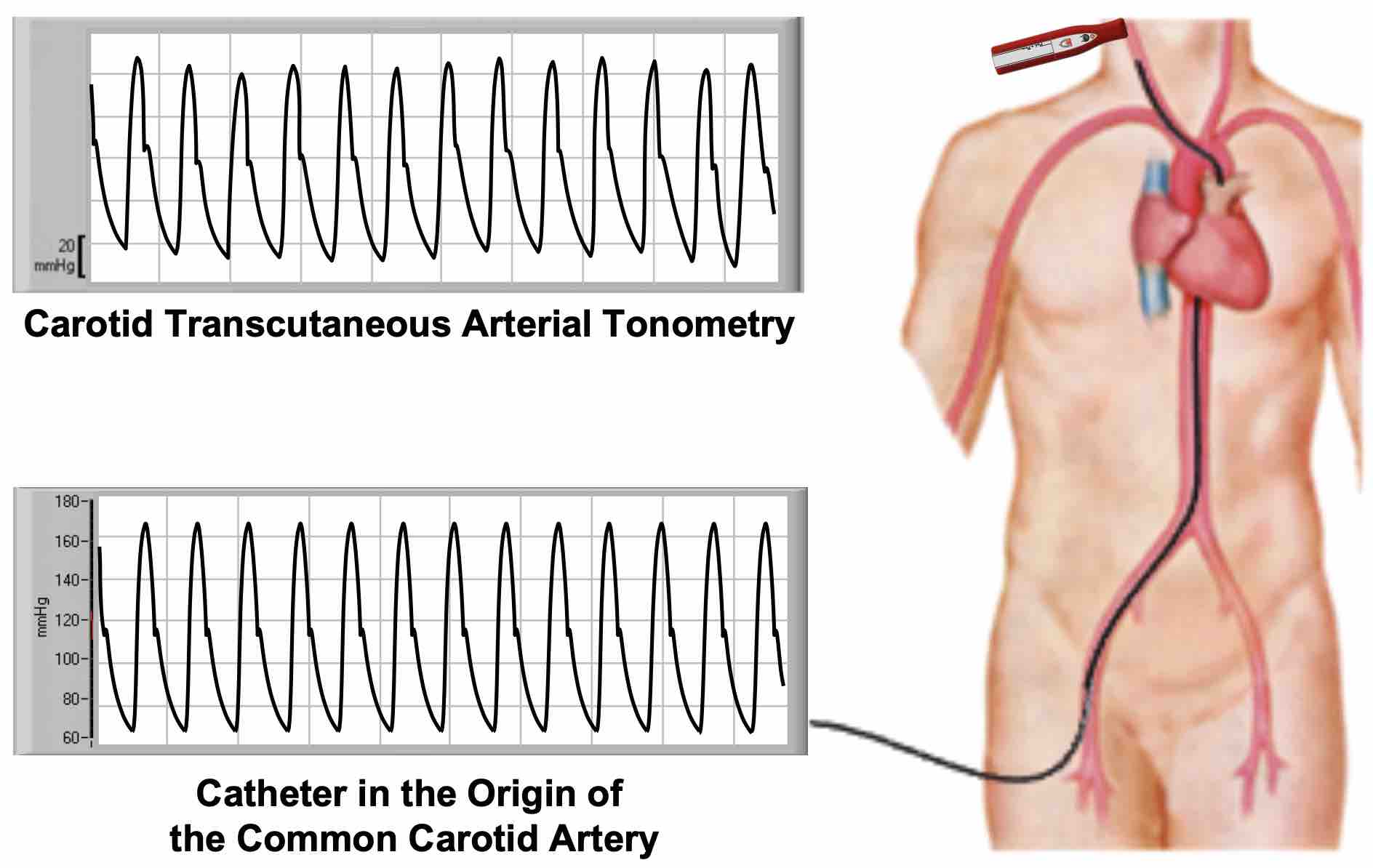
Non-invasive recordings of pressure waves provided by the PulsePen: comparison with invasive intra-arterial recordings1
The pressure waves assessed with the PulsePen on the carotid artery were compared with the intra-carotid pressure waves.1 The intra-arterial catheter was inserted into the origin of the common carotid artery and the transcutaneous tonometer probe simultaneously recorded the pulse pressure waves on the common carotid artery.
Invasive and non-invasive pressure waves were simultaneously recorded for a period of 10 s. Pressure wave signals were then split into harmonics. The evaluation was limited to the first six harmonics and was based on the Fourier analysis.1
The analysis of each harmonic confirmed that the two pressure waves, recorded invasively and non-invasively, were perfectly superimposable.
In a second step, the pressure waves assessed with the PulsePen on the carotid artery were compared with intra-aortic pressure waves.1 The intra-arterial catheter was placed at the origin of the ascending aorta and the transcutaneous tonometer probe on the common carotid artery.
The pressure waveforms obtained non-invasively with the PulsePen at the site of the common carotid artery were very similar to the aortic waveforms obtained invasively.1
Invasive and non-invasive pressure waves were nearly superimposable. The analysis of the first six harmonics showed only a slight, and insignificant, difference in the first harmonic of the pressure wave. However, the difference between the two pressure wave values was less than 5 mmHg.
The results of this study showed that the PulsePen is accurate in estimating central aortic pressure and pressure waveforms.
Non-Invasive estimation of aortic stiffness by PulsePen: comparison with invasive intra-aortic recordings 2
A study was designed to compare the "true" aortic PWV evaluated invasively through the gold standard approach based on an intra-aortic catheter, with that derived from a number of non-invasive devices available on the market for estimating aortic stiffness.2
The PWV was estimated with seven non-invasive devices (BPLab*, Complior-Analyse*, Mobil- O-Graph*, pOpmètre*, PulsePen-ET*, PulsePen-ETT* and SphygmoCor*) in 102 patients undergoing diagnostic coronary angiography. Non-invasive PWV data were compared with invasive aortic PWV.
Such a rigorous methodological approach yielded important findings:
1. Propagative methods including a large pathway of muscular arteries in the aortic pulse wave velocity assessment (pOpmètre) showed only a weak correlation with invasive estimates of aortic stiffness.
2. Algorithm-based systems (BPLab and Mobil-O-Graph) are closely linked to changes in age and blood pressure, thus these devices appear unable to detect a condition of early vascular aging.
3. Methods estimating carotid-femoral PWV (Complior-Analyse, PulsePen, SphygmoCor) should be considered the best non-invasive approach to reliably assess aortic stiffness, independently from other determinants.
Devices evaluating carotid-femoral PWV (Complior-Analyse, PulsePen-ET, PulsePen-ETT, SphygmoCor) showed a strong agreement between each other (r>0.83) and with invasive aortic PWV.
This table below shows the mean difference ± standard deviation (SD) with the invasive PWV:
The PulsePen (both ETT and ET model) showed the best agreement with the aortic invasive measurements.
Short-term repeatability of non-invasive aortic pulse wave velocity assessment: comparison between methods and devices 6
The accurate appraisal of repeatability is mandatory for a correct interpretation of the non-invasive PWV measurements.
Short-term repeatability of carotid-femoral PWV was estimated with different devices in 102 high cardiovascular risk patients.6 PWV was measured in a single session twice, at 15 minute interval, and its reproducibility was assessed though coefficient of variation (CV), coefficient of repeatability, and intraclass correlation coefficient.
Among the devices evaluated, the PulsePen demonstrated the best repeatability in the measurement of carotid-femoral PWV.
N, number of subjects; r, coefficient of correlation; CV, coefficient of variation with the relative 95% confidence interval; |d| absolute mean of differences ± standard deviation; CR, coefficient of repeatability; ICC, intraclass correlation coefficients with the relative 95% confidence interval.
Non-invasive estimation of Subendocardial Viability Ratio (SEVR) by PulsePen: validation versus invasive assessment 7
Estimation of the balance between subendocardial oxygen supply and demand could be a useful parameter to assess the risk of myocardial ischemia. Evaluation of the subendocardial viability ratio (SEVR, also known as Buckberg index) by invasive recording of left ventricular and aortic pressure curves represents a valid method to estimate the degree of myocardial perfusion relative to left ventricular workload. The introduction of arterial applanation tonometry for the recording of arterial pulse waves allowed a non-invasive estimation of SEVR. Different methods to estimate SEVR values with carotid applanation tonometry were compared with those evaluated invasively by cardiac catheterization.
The “traditional” method estimates the SEVR simply as the ratio between the areas below the central aortic pressure wave during diastole (myocardial oxygen supply) and during systole (myocardial oxygen demand), respectively. However, this “traditional” method does not take into account the intra-ventricular diastolic pressure and proper allocation to systole and diastole of left ventricular isometric contraction and relaxation, respectively, resulting in an overestimation of the SEVR values.
SEVR values acquired by invasive catheterization and transcutaneous carotid tonometry estimated by “traditional” method.
On the left, the scatter plots show linear correlation between SEVR values. Red dashed line represents the linear regression. On the right, Bland-Altman plot shows differences observed between SEVR values according to the average values. The area delimited by red dotted lines shows the mean values of differences (red dashed lines) ±1.96 standard deviation (SD) of mean SEVR values. DPTI, diastolic pressure-time index; SPTI, systolic pressure-time index.
This “traditional” method provided significantly higher SEVR values than the reference invasive SEVR: average of differences ±SD = 44% ±11% (limits of agreement: 23% to 65%).
The original method implemented in the PulsePen system was developed in an attempt to make the non-invasive SEVR estimate more concordant with the SEVR invasively measured by catheterization.
The PulsePen algorithm provides SEVR values taking into account all the main factors determining myocardial oxygen supply and demand, including left ventricular diastolic pressure, isovolumic contraction time and isovolumic relaxation time.
SEVR values acquired by invasive catheterization and transcutaneous carotid tonometry estimated by PulsePen.
On the left, the scatter plots show linear correlation between SEVR values. Red dashed line represents the linear regression. On the right, Bland-Altman plot shows differences observed between SEVR values according to the average values. The area delimited by red dotted lines shows the mean values of differences (red dashed lines) ±1.96 standard deviation (SD) of mean SEVR values. DPTI, diastolic pressure-time index; SPTI, systolic pressure-time index.
SEVR values provided by the PulsePen showed an excellent agreement with the invasive determination of SEVR: average of differences ±SD = 0.00 ±0.08 (limits of agreement: -0.15 to 0.16).
The accurate estimation of the subendocardial oxygen supply and demand balance could be a useful parameter to assess the risk of myocardial ischemia, particularly in those forms of myocardial damage that are not justified by overt coronary artery disease.
Validation of non-invasive estimation of Isovolumic Contraction Time (ICT) by PulsePen 8
PulsePen estimates isovolumic contraction time (ICT) from the time delay between the ‘R’ wave of the electrocardiogram and the foot of the carotid pulse waveform (RW), after adjustment for the pulse transit time from the aortic valve to the carotid artery site, evaluated by a validated algorithm based on the carotid-femoral pulse wave velocity (PWV).8
In order to validate the non-invasive estimation of ICT by means of arterial tonometry, the pulse waves were recorded by the PulsePen at the carotid artery simultaneously with the recording of the transvalvular aortic flow by Doppler echocardiography, synchronized by ECG gating.
ICT estimated by PulsePen was closely related to that measured by echocardiography, with homogeneous distribution in Bland-Altman analysis.8
Relationship between isovolumic contraction time (ICT) measured by echocardiography (echo ICT) and estimated values by PulsePen (tono ICT). White dots: healthy volunteers. Black dots: heart failure patients (HF) with reduced ejection fraction. Left panels: the scatterplots show linear correlation between the values where the dashed line represents the identity line. Right panels; the Bland-Altman analysis shows differences observed between the values obtained by the two methods as a function of their mean values. SD, standard deviation.
Non-invasive estimation of Left Ventricular Diastolic Pressure (LVDP) by PulsePen: validation versus invasive assessment 7
PulsePen estimates left ventricular mean diastolic pressure (LVDP) using a proprietary algorithm based on parameters derived from blood pressure values, patient anthropometric characteristics, and pulse waveform analysis.
The LVDP estimated by the PulsePen was compared with the real values of left ventricular diastolic pressure acquired simultaneously during ventricular catheterization.7
A good agreement between the estimated LVDP provided by the PulsePen tonometer software and the true one measured invasively was found.
Bland-Altman plot shows differences observed between LVDP values recorded by ventricular catheterization and estimated by PulsePen tonometer according to the average values. The area delimited by red dotted lines shows the mean values of differences (red dashed lines) ±1.96 standard deviation (SD) of mean SEVR values.
Confirming the robustness of the LVDP estimate by PulsePen, the differences in subendocardial viability ratio (SEVR) estimated with invasive catheterization and with carotid applanation tonometry by PulsePen device appears to be unrelated to an erroneous estimate of the LVDP.
Relationship between differences in subendocardial viability ratio (SEVR) estimated with invasive catheterization and with carotid applanation tonometry by PulsePen device and respective difference between left ventricular mean diastolic pressure (LVDP) measured with invasive and transcutaneous methods.
(*) All trademarks and brand names are the property of their respective owners.
References
1. Salvi P, Lio G, Labat C, Ricci E, Pannier B, Benetos A. Validation of a new non-invasive portable tonometer for determining arterial pressure wave and pulse wave velocity: the PulsePen device. J Hypertens 2004;22(12):2285-93.
2. Salvi P, Scalise F, Rovina M, Moretti F, Salvi L, Grillo A, Gao L, Baldi C, Faini A, Furlanis G, Sorropago A, Millasseau SC, Sorropago G, Carretta R, Avolio AP, Parati G. Noninvasive Estimation of Aortic Stiffness Through Different Approaches. Hypertension 2019;74(1):117-129.
3. Joly L, Perret-Guillaume C, Kearney-Schwartz A, Salvi P, Mandry D, Marie PY, Karcher G, Rossignol P, Zannad F, Benetos A. Pulse wave velocity assessment by external noninvasive devices and phase-contrast magnetic resonance imaging in the obese. Hypertension 2009;54(2):421-6.
4. Reference Values for Arterial Stiffness C. Determinants of pulse wave velocity in healthy people and in the presence of cardiovascular risk factors: 'establishing normal and reference values'. Eur Heart J 2010;31(19):2338-50.
5. Reusz GS, Cseprekal O, Temmar M, Kis E, Cherif AB, Thaleb A, Fekete A, Szabo AJ, Benetos A, Salvi P. Reference values of pulse wave velocity in healthy children and teenagers. Hypertension 2010;56(2):217-24.
6. Grillo A, Parati G, Rovina M, Moretti F, Salvi L, Gao L, Baldi C, Sorropago G, Faini A, Millasseau SC, Scalise F, Carretta R, Salvi P. Short-Term Repeatability of Noninvasive Aortic Pulse Wave Velocity Assessment: Comparison Between Methods and Devices. Am J Hypertens 2017;31(1):80-88.
7. Salvi P, Baldi C, Scalise F, Grillo A, Salvi L, Tan I, De Censi L, Sorropago A, Moretti F, Sorropago G, Gao L, Rovina M, Simon G, Fabris B, Carretta R, Avolio AP, Parati G. Comparison Between Invasive and Noninvasive Methods to Estimate Subendocardial Oxygen Supply and Demand Imbalance. J Am Heart Assoc 2021;10(17):e021207.
8. Salvi P, Grillo A, Tan I, Simon G, Salvi L, Gao L, Rovina M, Butlin M, Yang Y, Meneghin E, Meng L, Faini A, Barin E, Pini A, Carretta R, Huo Y, Avolio A, Parati G. Systolic time intervals assessed from analysis of the carotid pressure waveform. Physiol Meas 2018;39(8):084002.